Surgery
Lymph nodes are small bean shaped structures that are all over the body including near the breast. They are responsible for filtering the as it passes through them. The lymph nodes in the armpit (axilla) drain the lymphatic fluid from the breast and arm.
You might hear about different levels of lymph nodes. The lymph nodes in the axilla are divided into 3 groups. The group depends on where they are around the pectoralis minor muscle. This is the muscle that joins the ribs to the shoulder blade. The levels are:
level 1 nodes are closest to the breast - they are below or next to the muscle
level 2 nodes are behind the muscle
level 3 nodes are above the muscle near the collarbone
Breast cancer can spread to other parts of the body. If it does spread, it usually first spreads to the lymph nodes in the axilla.
It is important to know if there are cancer cells in the lymph nodes in the armpit and how many lymph nodes are affected. This helps the doctors work out the of your cancer and plan the best treatment for you.
Find out about staging breast cancer

You have an ultrasound scan of the lymph nodes under your arm at the same time as your other tests to diagnose breast cancer.
You usually have a biopsy of any lymph nodes that look abnormal. The biopsy is sent to the laboratory to check for cancer cells.
If this shows that the cancer has spread to the nodes in the armpit, you will have surgery to remove all or most of them. You have this at the same time as your breast surgery. This is called an axillary lymph node dissection (ALND) or clearance.
You have a sentinel lymph node biopsy instead if either the:
lymph nodes look normal during the ultrasound scan
results of an ultrasound guided biopsy shows no cancer cells
The sentinel node is the first lymph node in the armpit, where the fluid drains into from the breast. This means it’s the first lymph node the breast cancer could spread to.
Your surgeon usually carries out a sentinel lymph node biopsy during the operation to remove your breast cancer. You have about 1 to 3 nodes removed to see if they contain cancer cells.
You might have your sentinel lymph node biopsy with either:
a radiotracer and blue dye
the Magtrace and Sentimag system
A few hours before the operation, you have an injection of a small amount of mildly radioactive liquid into your breast close to the cancer. You usually have this in the nuclear medicine department in the hospital. The radioactive liquid is called a tracer.
During the operation, your surgeon may also inject a small amount of blue dye into the breast. The dye and the tracer drain away from the breast tissue into nearby lymph nodes.
The surgeon can see which group of lymph nodes the dye reaches first. They also use a radioactive monitor to see which group of lymph nodes the tracer gets to first.
The dye can stain your breast slightly blue. It gradually fades over a few weeks or months. The dye also turns your urine green for a few days.
In some hospitals surgeons use the Magtrace and Sentimag system to find sentinel lymph nodes.
Magtrace is a magnetic liquid tracer that is dark brown in colour. The surgeon injects the tracer into the breast tissue around the cancer. It acts as a magnetic marker and dye. The in the area soaks up the injected liquid and it gets trapped in the sentinel lymph nodes.
You can have Magtrace up to 30 days before your operation.
During your operation the surgeon uses a probe called a Sentimag to detect the magnetic liquid trapped in the sentinel lymph nodes. The liquid also acts like a brownish dye so the surgeon can see where it is trapped. The surgeon can then remove the sentinel lymph nodes for testing.
The surgeon usually removes about 1 to 3 of these nodes. They might remove other lymph nodes if they look as though they might contain cancer cells. They send the nodes to the laboratory to check for cancer cells. The results can take a few weeks.
If none of the lymph nodes contain cancer cells, you won’t need to have any more nodes taken out.
If there are cancer cells in the sentinel nodes you usually need more treatment. You may have another operation to remove most or all of the lymph nodes under your arm. This is called axillary lymph node dissection or axillary clearance. This is generally about 2 weeks after you get the results.
Radiotherapy means the use of radiation, usually x-rays, to treat cancer. Some people have radiotherapy to the armpit to destroy any remaining cancer cells instead of surgery.
Read about radiotherapy for breast cancer
In some hospitals, the surgeon gets the results of the sentinel lymph node biopsy during the operation. They can then remove the rest of the nodes (axillary lymph node dissection) if necessary. You then avoid having a second operation. This type of testing is called one step nucleic acid amplification (OSNA).
Your surgeon will explain this to you before your operation, so you know what to expect.
You might have lymph nodes removed as part of your breast surgery or as a separate operation.
You have a general anaesthetic for the operation, so you will be asleep the whole time.
The surgeon makes a small cut in your armpit to remove the lymph nodes. Generally, they remove between 10 and 15 lymph nodes. But the number of nodes in the armpit varies from person to person.
The surgeon sends the lymph nodes to the laboratory to check them for cancer cells. You get the results at your follow up appointment.
After the operation, you usually wake up in the recovery room before moving back to your ward or day unit. Find out what else to expect immediately after surgery.
You have follow up appointments to check your recovery and sort out any problems. They are also your opportunity to raise any concerns you have.
You usually see your surgeon one to two weeks after your operation. They examine you and check your wound is healing well.
Your surgeon will explain the results of your surgery and talk about any further treatment you might need.
You'll have contact details of your breast care nurse or the ward if you need to contact someone before your follow up.
There are some possible problems after having surgery to the lymph nodes in your axilla. Not everyone will have these but there is a bigger risk if you have an axillary dissection. Some of these problems include:
You are at risk of long term swelling (lymphoedema) in your hand and arm after surgery to remove the lymph nodes in your armpit. This is swelling caused by lymph fluid that can't drain away. It can happen any time after surgery or radiotherapy to your armpit.
Not everyone will get this and it is less likely to happen if you only have a few nodes removed. But it is very important to speak to your specialist nurse or surgeon if you think your arm or hand may be swollen.
Unfortunately, once you have lymphoedema it can’t be cured. But early treatment can help to control it. Your nurse will talk to you about ways of preventing lymphoedema.
Find out about lymphoedema after breast cancer treatment
Your shoulder might become stiff and painful after breast surgery to the lymph nodes. Your nurse or a physiotherapist will show you exercises to do after your operation to help improve movement in the shoulder.
Find out about exercise after breast surgery
Sometimes fluid collects near the wound and around the armpit. This might happen after your nurse removes the wound drain if you have one.
It can cause:
swelling
pain
an increased risk of infection
The fluid normally goes away on its own within a few weeks.
Your nurse or doctor can drain the fluid with a needle and syringe if the seroma is painful. Sometimes the fluid can build up again after being drained.
Tell your doctor or nurse if you think a seroma is developing.
Tell your doctor or nurse if your wound:
looks red and swollen
feels warm
is painful
leaks fluid (discharge)
These are signs of infection. You may also feel unwell and have a temperature.
If you have an infection, your doctor will give you antibiotics. You might need to go back into hospital or stay in longer if you need antibiotics through a drip.
You might have numbness, tingling or a shooting pain in your armpit, upper arm, shoulder or chest wall. This is due to damage to the nerves during surgery. The nerves usually repair themselves, but it can take many weeks or months.
Your doctor or nurse can give you medicines to help with nerve pain.
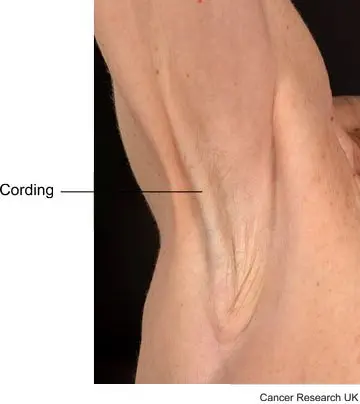
Some women develop scar tissue in the armpit after lymph node removal. The connective tissues in the armpit get inflamed, which forms one or more tight bands. This usually happens within the first few weeks or months after the operation.
The scar tissue is called cording, banding or axillary web syndrome. It can feel something like a guitar string. It can extend down the arm past the elbow, possibly as far as the wrist or thumb.
Cording is harmless but can be painful and may limit your arm movement. Massaging the area regularly can help. Tell your breast care nurse if you develop cording. They can refer you to a physiotherapist. They can show you how to massage the area and teach you stretching exercises. It usually gets better within a few months. Taking anti inflammatory painkillers may also help. Speak to your nurse or doctor about taking these.
Last reviewed: 10 Jun 2026
Next review due: 11 Jun 2029
Before your operation for breast cancer you have tests to check your fitness and you meet members of your treatment team. Find out what happens before you operation.
On the day of your breast surgery you will need to stop eating for several hours beforehand surgery. Find out what else happens before you go to theatre for your breast surgery.
Read about what happens after breast surgery, exercises you need to do, and how to cope with possible problems.
After breast cancer surgery your physiotherapist or breast care nurse will ask you to do regular arm and shoulder exercises.
Getting practical, physical and emotional support can help you to cope with a diagnosis of breast cancer. It can also help you with life during and after treatment.
Breast cancer is cancer that starts in the breast tissue. It’s the most common cancer in the UK. It mainly affects women, but men can get it too.
About Cancer generously supported by Dangoor Education since 2010. Learn more about Dangoor Education


Search our clinical trials database for all cancer trials and studies recruiting in the UK.
Connect with other people affected by cancer and share your experiences.
Questions about cancer? Call freephone 0808 800 40 40 from 9 to 5 - Monday to Friday. Alternatively, you can email us.